
Savonia Article Pro: When One Dose Goes Wrong: Understanding Medication Errors in Finnish Healthcare System
Savonia Article Pro is a collection of multidisciplinary Savonia expertise on various topics.
This work is licensed under CC BY-SA 4.0![]()
![]()
![]()
Although medicines are used to improve health, they can sometimes lead to unintended harm. Mistakes and medication use are not always immediately visible, yet their effect can be serious. A single mistake in prescribing or missed followed up step can lead to serious injury or even death. (World Health Organization WHO, 2019, 2024; Linden-Lahti et al., 2021).

Research shows that such errors are not rare but occur as part of everyday health care practice.
This article examines the underlying causes of medication errors in Finland, and how understanding these situations can improve patient safety, particularly for future healthcare professionals. (Linden-Lahti et al., 2021; Linden-Lahti, 2023.)
In Finland, medication errors are among the most reported patient safety incidents. Studies show that over half of the most serious cases have led to permanent harm or even death. These situations rarely rise from simple carelessness. Instead, they are typically connected to border system-level factors that influence how healthcare work is carried out. (Linden-Lahti et al., 2021.)
The aim of this article is to provide a clear focused understanding of why Medication errors occur, what factors increase their risk, and how they can be prevented special attention is giving to system level challenge high risk situation and practical role of healthcare professionals and improving safety.
UNDERSTANDING MEDICATION ERRORS IN PRACTICE
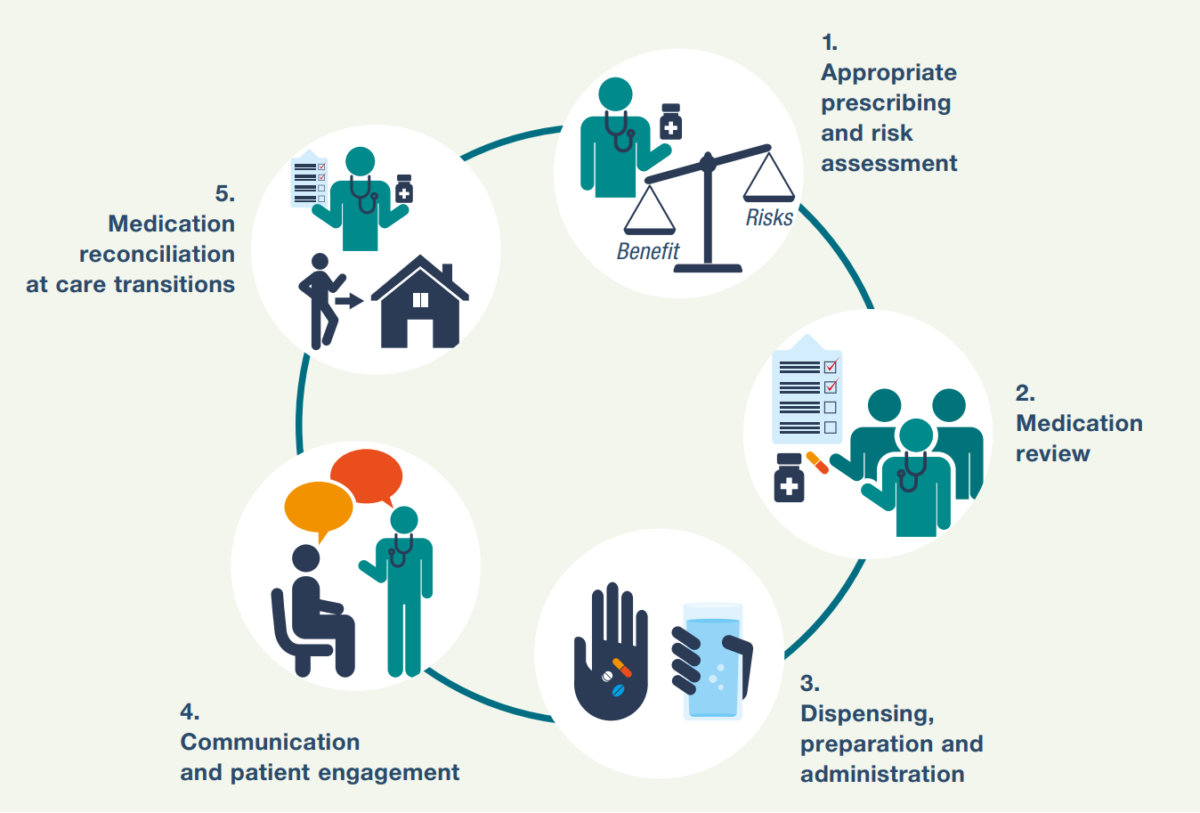
A medication error is generally defined as preventable event that may lead to inappropriate medication use or patient harm. These errors can occur at any stage of the medication process, including prescribing, dispensing, administration, and monitoring. (World Health Organization WHO, 2024.) While some errors seem minor, they can still affect recovery, especially in patients with complex health conditions. (Vellonen et al., 2025.)
Although some errors may appear minor, their effects can be significant, particularly for patients with complex conditions. For example, an incorrect dose in an elderly patient with multiple illnesses may lead to complications that are not immediately recognized. Research conducted in Finland shows that medication errors are often linked to working conditions rather than individual mistakes. Interruptions, unclear instructions, and high workload all increase the likelihood of errors in routine care. (Härkänen, 2014; Vellonen et al., 2025.)
WHAT SERIOUS CASES IN FINLAND REVEAL
Studies based on reports to Finnish supervisory authorities provide valuable insight into the nature of severe medication errors. These cases rarely result from a single mistake. Instead, they typically develop through a chain of small failures occurring at different stages of care. For instance, an incorrect prescription may go unnoticed during dispensing, and the patient’s condition may not be monitored closely enough afterwards. Overtime, this accumulation of errors across the care process demonstrates how risks can escalate when communication and monitoring systems fail simultaneously. (Linden-Lahti et al., 2021.)
Older adults are particularly vulnerable in these situations. A large proportion of serious cases involve individuals over the age of 60. This is largely due to polypharmacy, where patients use multiple medications (five or more) simultaneously. While necessary for managing chronic conditions, polypharmacy increases the risk of drug interactions and makes the treatment more complex. As a result, careful monitoring and clear communication become even more important. (Linden-Lahti et al., 2021; Linden-Lahti, 2023.)
Errors in prescribing are frequently the starting points in these situations. Problems such as Incorrect dosing, unclear instructions, or unsuitable medication choices can Initiate the chain of events that is difficult to stop. At the same time, insufficient follow up may prevent early detection of complications, allowing the situation to worsen unnecessarily. (Härkänen, 2014; Linden-Lahti et al., 2021.)
HIGH-RISK MEDICATIONS AND PATIENT GROUPS
Certain types of medications are more Frequently associated with serious errors these include medicines affecting blood clotting, strong pain medications, and drugs used in mental health require careful attention. Such medications have a small safety margin, meaning that even small deviations in their use can lead to severe consequences. (Linden-Lahti et al., 2021; Linden-Lahti, 2023.)
The environment in which care is provided also plays a role. In home care and long-term care settings patients are often treated by several professionals. Information does not always transfer smoothly between them, which can lead to misunderstandings or missing details. Even when each professional acts carefully, gaps in communication can create situations where errors occur despite careful intensions. (Laatikainen et al., 2020; Finnish Supervisory Agency, 2023.)
WHY DO ERRORS CONTINUE TO HAPPEN
Medication errors are rarely the result of simple carelessness, instead closely linked to the way healthcare systems are organized. Factors such as unclear documentation, fragmented communication and lack of coordination between professionals all contribute to risk. In addition, healthcare professionals often work under pressure, managing multiple tasks at the same time. This increased cognitive load and makes errors more likely, especially in demanding situations. (Linden-Lahti, 2023; World Health Organization WHO, 2024.)
Communication remains one of the most significant challenges. If medication information is incomplete or unclear it can easily be misunderstood. Similar drug names or packaging can also lead to confusion, particularly in busy environments. These issues highlight the importance of clear and consistent communication practices in all areas of care. In addition, incidents reporting systems may not capture all errors, as I underreporting is common due to time constraints or fear of blame, which can limit the full understanding of the problem. (Härkänen, 2014; Laatikainen et al., 2020; Linden-Lahti et al., 2021; Linden-Lahti, 2023.)
LEARNING CULTURE INSTEAD OF BLAME
Finnish healthcare has increasingly shifted toward a culture that focuses on learning rather than blaming individuals. The focus is on identifying underlying causes and improving systems rather than assigning individual blame. (Linden-Lahti, 2023; World Health Organization WHO, 2024.)
Reported incidents have already led to practical improvements, such as clearer guidelines, better communication methods, and wider use of digital tools. These changes show that when errors are addressed constructively, they can lead to meaningful and lasting improvement in patient safety. This approach also reflects ethical principles in healthcare where patient safety and transparency are prioritized over punishment. (Linden-Lahti et al., 2021; Finnish Supervisory Agency, 2023; Linden-Lahti, 2023.)
IMPROVING SAFETY IN PRACTICE
Improving medication safety requires both individual responsibility and system level support. Finnish research highlights the following approaches are essential:
- Strengthening prescribing practice and ensuring clarity and medication orders.
- improving communication between healthcare professionals.
- increasing monitoring and follow-up of patients.
- paying special attention to high-risk medications.
- supporting staff competence and reducing workload-related stress.
Developing a strong safety culture is also critical. When professionals feel safe reporting errors, organizations gain valuable information that can be used to improve care. (Härkänen, 2014; Linden-Lahti et al., 2021.)
Education and simulation training help professionals prepair for real situations. While digital tools, such as electronic medication systems and the smart medication cabinets can reduce the risk of manual error. However, technology alone is not enough. Safe practice ultimately depends on professional judgment, teamwork, and the sense of responsibility. (Finnish Supervisory Agency, 2023; World Health Organization WHO, 2024.)
RELEVANCE FOR FUTURE HEALTHCARE PROFESSIONALS
For nursing students and other health care professionals, understanding medication errors is an essential part of developing clinical competence. These situations are not rare exceptions but part of everyday health care work. Recognizing potential risk and knowing how to respond to them are critical skills in ensuring patient safety. (Linden-Lahti et al., 2021; World Health Organization WHO, 2024.)

Safe medication use is also an ethical responsibility. Every prevented error contributes directly to better patient outcomes and improved quality of care. By developing awareness, applying evidence-based knowledge, and supporting a culture of safety, future professionals can play an important role in reducing medication errors and strengthening health care systems. (World Health Organization WHO, 2019, 2024; Finnish Supervisory Agency, 2023.)
Writers
Author: Ali Al-Rufaye, Nursing Student, ali.al-rufaye@edu.savonia.fi
Supervisor: Leena Koponen, Senior Lecturer, leena.koponen@savonia.fi
International Unit of Health Care, International Degree Programmes, Unit of International Affairs
References
Härkänen, M. (2014). MARJA HÄRKÄNEN Medication-related Adverse Outcomes and Contributing Factors among Hospital Patients. Link: https://erepo.uef.fi/items/a5a565c3-ce84-42cc-853b-14d7802cf388.
Laatikainen, O., Sneck, S., & Turpeinen, M. (2020). The risks and outcomes resulting from medication errors reported in the Finnish tertiary care units: A cross-sectional retrospective register study. Frontiers in Pharmacology, 10. https://doi.org/10.3389/fphar.2019.01571. Accessed 06/04/2026.
Linden-Lahti, C. (2023). SEVERE MEDICATION ERRORS – A CHALLENGE FOR PATIENT SAFE-TY. https://helda.helsinki.fi/items/d404f9ec-78e7-4d7e-b26f-29bb173ed3da.
Linden-Lahti, C., Takala, A., Holmström, A. R., & Airaksinen, M. (2021). What severe medication errors reported to health care supervisory authority tell about medication safety? Journal of Patient Safety, 17(8), E1179–E1185. https://doi.org/10.1097/PTS.0000000000000914
Finnish Supervisory Agency. (2023). Valviran tilinpäätös ja toimintakertomus 2023. https://lvv.fi/documents/242146171/248315744/Valvira-toimintakertomus-2023.pdf/7a8880ce-b3d2-5996-f6c6-6680af8d8d0c/Valvira-toimintakertomus-2023.pdf?t=1767173323409.
Vellonen, M., Härkänen, M., & Välimäki, T. (2025). Flow of Medication Information Incidents in the Home Care Setting in Finland: A Qualitative Descriptive Study. Journal of Advanced Nursing. https://doi.org/10.1111/jan.70063. Accessed 07/04/2026.
World Health Organization WHO. (2019). Medication Safety in Polypharmacy. http://apps.who.int/bookorders. Accessed 06/04/2026.
World Health Organization WHO. (2024). Global Burden of Preventable Medication-Related Harm in Health Care: A Systematic Review. World Health Organization. https://www.who.int/publications/i/item/9789240088887. Accessed 05/04/2026.
Image 1: Medication dosette. Source: AI-generated image (ChatGBT/OpenAI)
Image 2: Medication Safety in Polypharmacy (WHO, 2019).
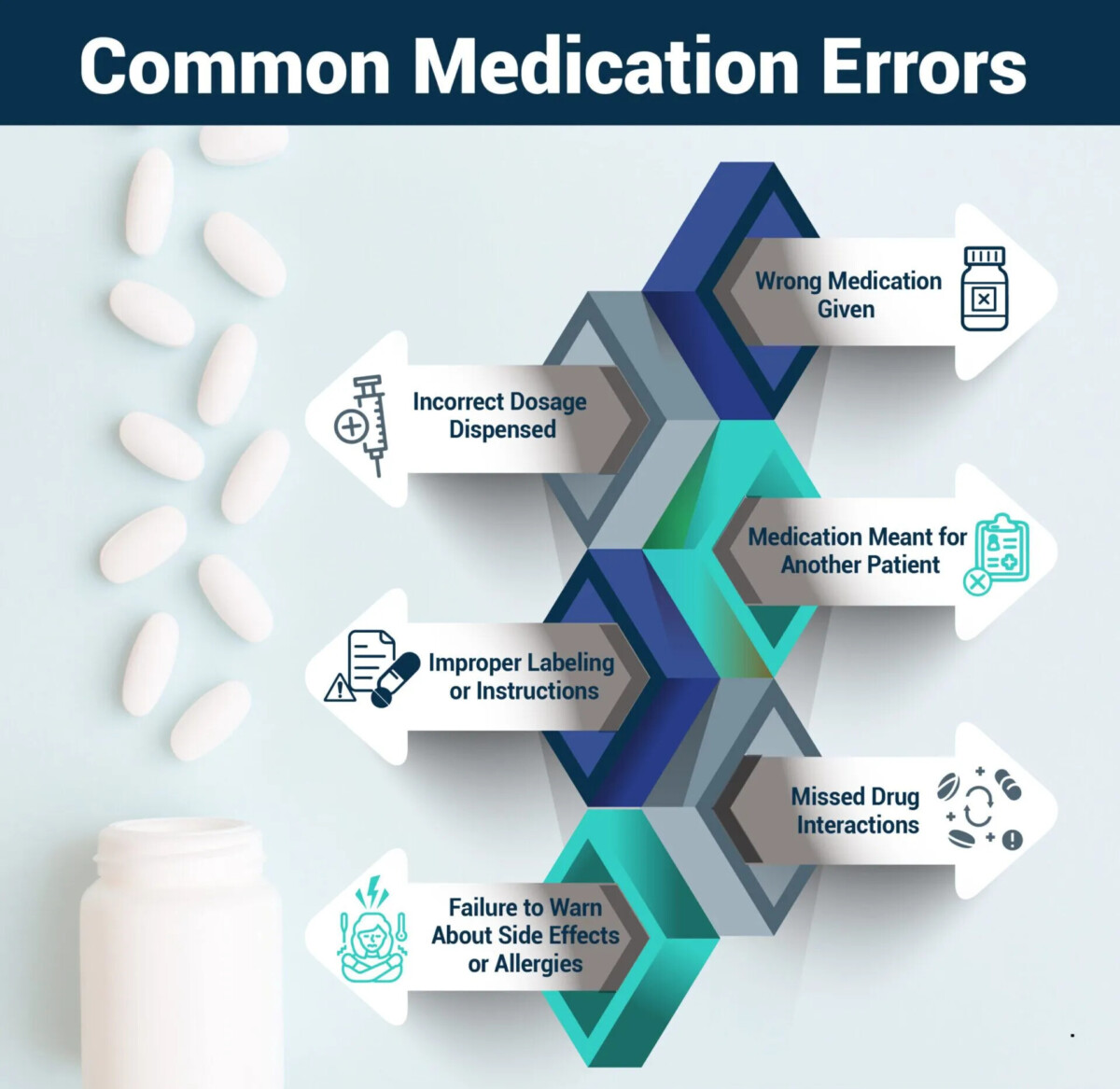
Image 3: Common Medication Errors, Source https://warnetthallen.com/pharmacy-malpractice-and-medication-errors
Image 4: Despensing Medications. Source https://resolution.nhs.uk/2023/03/30/learning-from-medication-errors/